

One pertinent question anyone opening a medical spa or healthcare practice must ask themselves is, “Who can do what?” Medical Professionals operating outside of their scope of practice, is one of the major legal pitfalls practices often find themselves falling into. This could result in lawsuits, problems with the regulatory authorities in their state, and harm to the reputation of their business.
The scope of practice for medical professionals is highly regulated, making it easy to get confused about what is and is not allowed. Such regulations vary state by state, are constantly being changed, and are often located in multiple sources. This article will provide a brief overview of the regulation of NPs and then break down what the scope of practice is for a Nurse Practitioner (NP) by category, for each US state, as referenced by the American Association of Nurse Practitioners. This is a snapshot of information as of August 4, 2021, about where a NP can operate independently and where physician supervision is still needed. This article is not intended to be advertising or legal advice and is for informational purposes only.
Overview of the Regulation of Nurse Practitioners
The scope of practice for NPs is wide and varied across states because of a decades long debate of whether educational gaps between NPs and physicians render NPs unsafe and unqualified to care for patients independently.
In order to become a NP, candidates must complete a master’s or doctoral degree program and have advanced clinical training beyond that initially acquired as a registered nurse. Research has been published showing NPs can provide safe, high-quality, and cost-effective care equal to that of physicians and help close the widening gap between an ample number of providers to patients. Because of this, more and more states have been granting NPs independence to provide medical care without oversight or management of a physician.
Some states, however, still believe NPs should not be allowed to practice autonomously and require complete supervision or reduced authority to practice.
Current Breakdown of Regulations
The American Nurses Association defines scope of practice as “the services that a qualified health professional is deemed competent to perform and permitted to undertake — in keeping with the terms of their professional license.”
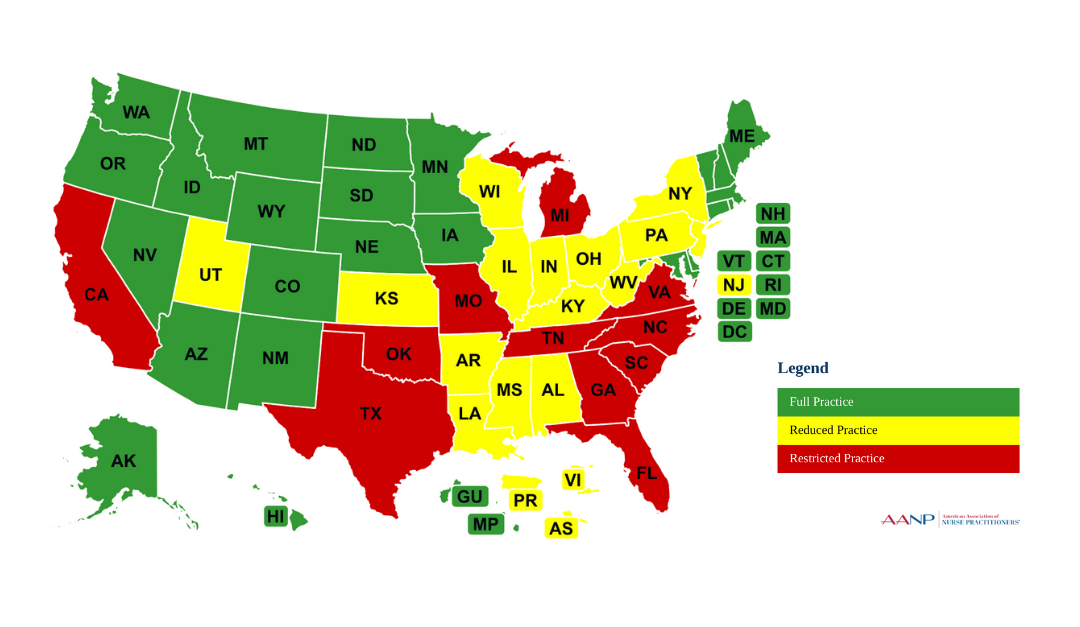
The American Association of Nurse Practitioners has broken down the scope of practice for NPs into three categories: Full, Reduced, and Restricted.
Full Practice
State practice and licensure laws permit all NPs to evaluate patients; diagnose, order and interpret diagnostic tests; and initiate and manage treatments, including prescribing medications and controlled substances, under the exclusive licensure authority of the state board of nursing. This is the model recommended by the National Academy of Medicine, formerly called the Institute of Medicine, and the National Council of State Boards of Nursing.
Reduced Practice
State practice and licensure laws reduce the ability of NPs to engage in at least one element of NP practice. State law requires a career-long regulated collaborative agreement with another health provider in order for the NP to provide patient care, or it limits the setting of one or more elements of NP practice.
Restricted Practice
State practice and licensure laws restrict the ability of NPs to engage in at least one element of NP practice. State law requires career-long supervision, delegation or team management by another health provider in order for the NP to provide patient care.
Source: “State Practice Environment.” American Association of Nurse Practitioners, AANP, 4 Aug. 2021, www.aanp.org/advocacy/state/state-practice-environment. (see also interactive state map)
Full Practice States include: Alaska, Arizona, Colorado, Connecticut, District of Columbia, Hawaii, Idaho, Iowa, Maine, Maryland, Massachusetts, Minnesota, Montana, Nebraska, Nevada, New Hampshire, New Mexico, North Dakota, Oregon, Rhode Island, South Dakota, Vermont, Washington, and Wyoming.
Reduced Authority States include: Alabama, Arkansas, Delaware, Illinois, Indiana, Kansas, Kentucky, Louisiana, Mississippi, New Jersey, New York, Ohio, Pennsylvania, Utah, West Virginia, and Wisconsin
Restricted Authority States include: California, Florida, Georgia, Michigan, Missouri, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, and Virginia.
Looking Forward
As shown by the breakdown of states above, the scope of authority for NPs throughout the US is still very much divided, leaving this area of regulation unsettled and shifting. Despite the full practice model being recommended by the National Academy of Medicine, formerly called the Institute of Medicine, and the National Council of State Boards of Nursing, 27 states are still operating under a reduced or restricted scope of practice.
While the debate around what should be an NP’s scope of practice continues, medical spa owners and managers need to look closely at the laws of the state they operate in to ensure their compliance with the applicable regulations. Do NP’s have full practice authority? Can they own their own practice? If their scope of practice is reduced or restricted, what is reduced or restricted?
At Lengea, we provide assistance with challenging questions like this and can quickly help you navigate this rapidly changing landscape. Contact us today for a free 15-minute consultation.